Annual Physical Examination Template in PDF
Annual Physical Examination Template in PDF
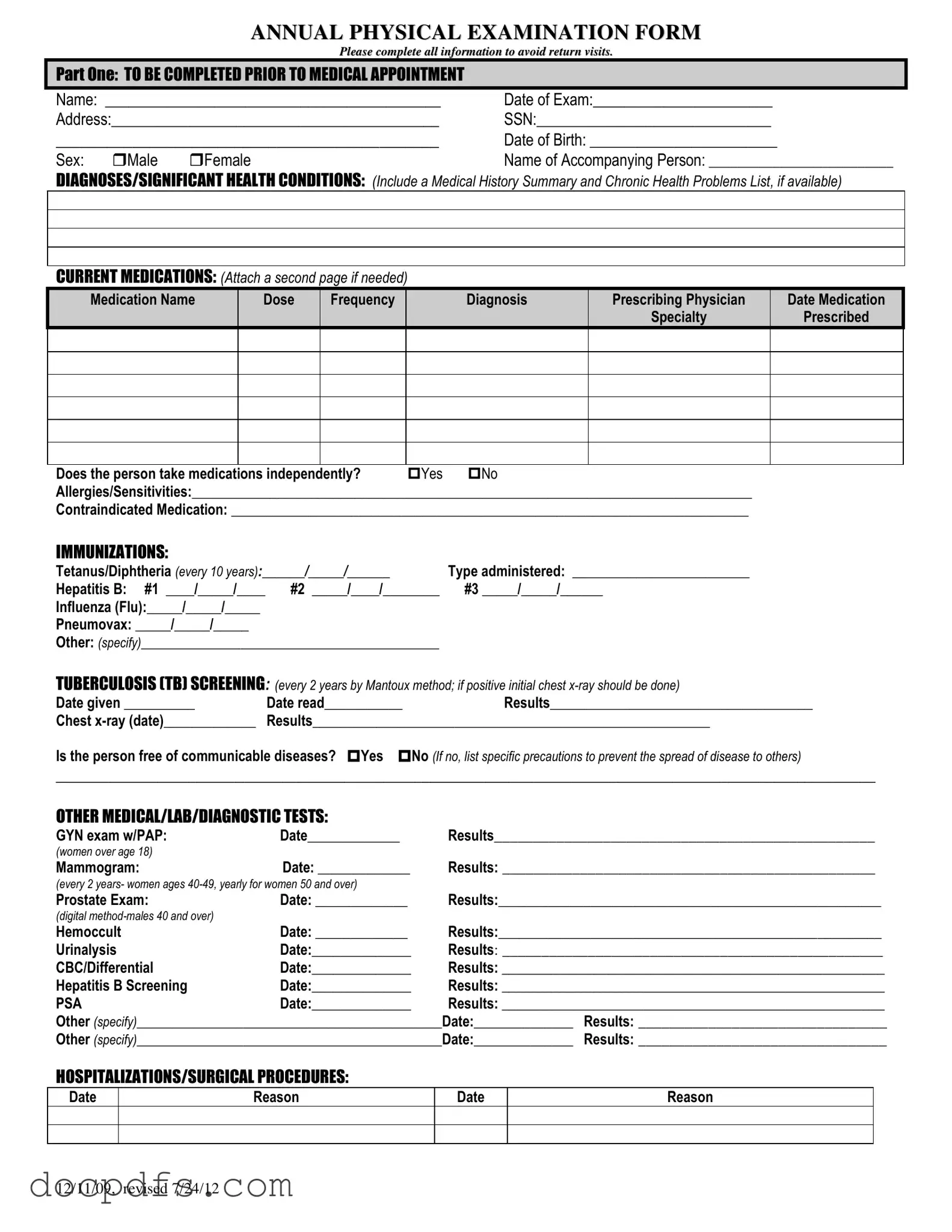
The Annual Physical Examination form serves as a comprehensive tool designed to gather essential health information prior to a medical appointment. It begins with basic personal details, including the individual's name, date of birth, and contact information. This section ensures that the healthcare provider has accurate data to reference. Next, the form requires a summary of any significant health conditions and a list of current medications, which helps the physician understand the patient's medical history and ongoing treatments. It's important to note any allergies or sensitivities, as this information can significantly impact treatment decisions. Additionally, the immunization history is recorded, detailing vaccinations such as Tetanus, Hepatitis B, and Influenza, which are crucial for preventive care. The form also includes a section for tuberculosis screening and other diagnostic tests, ensuring that any necessary evaluations are documented. Furthermore, a general physical examination section captures vital signs and assessments of various body systems, allowing for a thorough review of the patient's health status. Finally, there are spaces for additional comments and recommendations, ensuring that the physician can provide tailored advice for health maintenance and any required follow-ups. Completing this form accurately is vital to facilitate an effective and efficient medical visit.
Dnd Fillable Character Sheet - Outline your character's charisma for social interactions.
Lyft Driver Number - Ensure your vehicle's registration and insurance are current.
For parents navigating financial responsibilities, the Child Support Texas form serves as an essential tool, guiding them through the requirements of child support. It is important for parents to familiarize themselves with the terms laid out in the form, which can be accessed conveniently at https://texasformsonline.com/free-child-support-texas-template/, to ensure compliance and support their children effectively.
Ms Word Chart Examples - Column 1: Overview of findings or themes discussed in the topic.
The Annual Physical Examination form is a vital document for assessing an individual's health status. Along with this form, several other documents are commonly utilized to ensure a comprehensive evaluation. Each of these documents serves a specific purpose in the healthcare process.
Utilizing these documents alongside the Annual Physical Examination form creates a well-rounded approach to patient care. Each form contributes to a clearer understanding of the individual's health, enabling healthcare providers to make informed decisions.
Things to Do:
Things to Avoid:
When filling out the Annual Physical Examination form, it is important to ensure accuracy and completeness. Here are some key takeaways to keep in mind:
Completing the Annual Physical Examination form is an important step in ensuring that your health needs are accurately documented and addressed. After filling out this form, you will be prepared for your medical appointment, allowing your healthcare provider to better understand your medical history and current health status. Follow these steps carefully to ensure all required information is provided.
The Annual Physical Examination form is designed to gather essential health information about an individual prior to their medical appointment. This information helps healthcare providers assess the patient’s overall health, identify any existing conditions, and plan appropriate care. Completing this form thoroughly can minimize the need for follow-up visits, ensuring a more efficient healthcare experience.
Part One of the form requires personal details such as the patient's name, date of birth, address, and Social Security Number. Additionally, it asks for information about current medications, allergies, immunizations, and any significant health conditions. Providing a complete medical history summary and a list of chronic health problems is also encouraged to give the healthcare provider a clearer picture of the patient's health status.
When listing current medications, include the medication name, dosage, frequency of intake, the diagnosis for which it was prescribed, the prescribing physician's name, and the date it was prescribed. If you are taking multiple medications, feel free to attach an additional page if necessary. It is also important to indicate whether the individual takes medications independently.
The form requires documentation of several immunizations, including:
Any additional immunizations should also be specified. Keeping this information up to date is crucial for preventive health measures.
If you have allergies or sensitivities, you should clearly list them in the designated section of the form. This information is vital for healthcare providers to avoid prescribing medications or treatments that could trigger an allergic reaction. Additionally, if there are any contraindicated medications, those should also be noted to ensure patient safety.
If you have a history of communicable diseases, you must indicate this on the form. You will also need to specify any precautions that should be taken to prevent the spread of disease to others. This information allows healthcare providers to take necessary steps to protect both the patient and others in the healthcare setting.
Part Two focuses on the general physical examination. It includes vital signs such as blood pressure, pulse, and temperature, as well as a comprehensive evaluation of various body systems. The healthcare provider will assess whether findings are normal and may provide comments or recommendations for further evaluation if necessary. This section helps in identifying any immediate health concerns that may require attention.