Medication Administration Record Sheet Template in PDF
Medication Administration Record Sheet Template in PDF
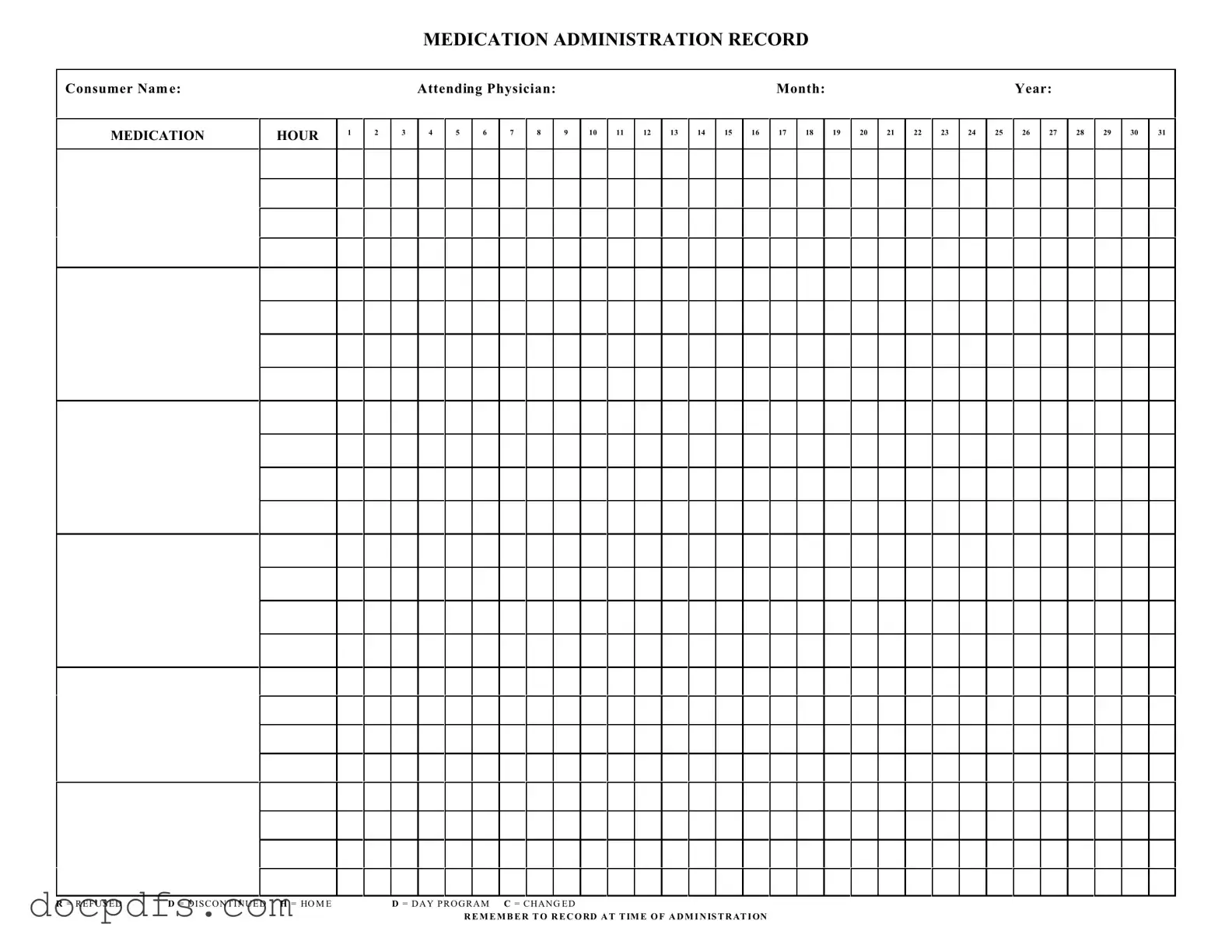
The Medication Administration Record Sheet is an essential tool in healthcare settings, particularly for ensuring that patients receive their medications safely and accurately. This form includes key details such as the consumer's name, the attending physician, and the month and year for proper documentation. It features a structured grid where healthcare providers can record the administration of medications at various hours throughout the day. Each hour is clearly marked, allowing for easy tracking of medication schedules. Additionally, the form includes specific notations, such as "R" for refused, "D" for discontinued, "H" for home, "D" for day program, and "C" for changed, which help in communicating important changes in a patient's medication regimen. It is crucial to remember to record the time of administration, as this ensures that all medication is given as prescribed and helps maintain an accurate medical history for each consumer.
CBP Declaration Form 6059B - All travelers should familiarize themselves with this important form.
How to Calculate Electrical Load of a House in India - Users must provide details about the planned electrical installations.
When completing a transaction involving a dirt bike, it is important to utilize the Dirt Bike Bill of Sale form, which provides a clear record of the ownership transfer. This legal document not only serves as proof of sale but also outlines essential details about both the buyer and the seller. For more information and to access the form, you can visit New York PDF Docs, ensuring a smooth and legitimate transaction.
Notice of Intent to Lien Florida - Contractors should be diligent in sending this notice to protect their financial interests.
The Medication Administration Record Sheet is an essential tool in healthcare settings, particularly for tracking patient medication. However, several other forms and documents complement this record, ensuring a comprehensive approach to patient care. Below is a list of commonly used documents that work alongside the Medication Administration Record Sheet.
Each of these documents plays a vital role in ensuring safe and effective medication administration. Together, they create a framework that supports both healthcare providers and patients in achieving the best possible outcomes.
When filling out the Medication Administration Record Sheet form, it's essential to ensure accuracy and clarity. Here are five important dos and don'ts to keep in mind.
Here are some key takeaways for filling out and using the Medication Administration Record Sheet form:
Remember to record all information at the time of administration to maintain accuracy.
Filling out the Medication Administration Record Sheet is essential for accurately tracking medication administration for individuals. This form helps ensure that all medications are given as prescribed and that any changes or refusals are properly documented. Below are the steps to complete the form effectively.
The Medication Administration Record Sheet (MARS) is used to document the administration of medications to consumers. It helps ensure that medications are given as prescribed by the attending physician. This record allows caregivers and healthcare providers to track which medications have been administered, refused, or discontinued, thus promoting safety and accountability in medication management.
To complete the MARS, follow these steps:
Caregivers, nurses, or healthcare providers who administer medications are responsible for maintaining the MARS. They must ensure that the record is accurately filled out and updated in real-time. This responsibility is vital for ensuring that all healthcare team members are informed about the consumer's medication status.
If a medication is refused or discontinued, the responsible caregiver should mark the appropriate letter in the MARS. Additionally, it is important to document the reason for refusal or discontinuation in a separate note or section, if available. This information can be critical for ongoing care and should be communicated to the healthcare team.
The MARS enhances medication management by providing a clear and organized way to track medication administration. It helps prevent medication errors, ensures compliance with prescribed regimens, and facilitates communication among healthcare providers. By maintaining accurate records, caregivers can identify patterns in medication administration and make informed decisions regarding the consumer's care.